50Y/F PRESENTED WITH SLURRING OF SPEECH.
History of present illness
Patient was apparently asymptomatic 3 months ago ,then she developed slurring of speech which was preceded by history of head trauma (fall onto door) For 2 days she complained of slurring of speech which improved gradually
History of weakness and tingling of all4 limbs, delayed response to normal stimuli, decreased memory and episodes of giddiness one month ago
22 days ago @ 3:30 am attenders had noticed staring eye movements which lasted for 15 mins, which was loss of consciousness, uprolling of eyes, stiffness of all 4 limbs frothing at mouth , post ictal confusion lasted for 30 mins
6 days ago attenders had noticed staring eye movements which lasted for 10 mins which was loss of consciousness , stiffness of all 4 limbs, involuntary micturition ,clenching of teeth post ictal confusion lasted for 20 mins
Past history;
Not a known case of DM HTN TB asthma thyroid disorders
From 22 days she was complaining of slurring of speech
No history of vomitings ,loose stools , fever, and pain abdomen
History of electric shock 6 years ago
History of burning micturition cold and cough 6 years
Personal history;
Married
Diet mixed
Apatite_ lost. takes food when the family member provided
Micturation is normal
No known allergies
Habits .no addictions
MENSTRUAL HISTORY;
Menopause 4years ago
Family history;
No relavent history is found
General examination;
Patient is conscious,coherent,cooperative



EXAMINATION
BP:140/100mm hg
PR:90bpm
RR:16/min
Temp : Afebrile
CNS:
Pupils- left- normal in size reactive to light
right-NSRL
Higher mental functions
- Conscious +
- Memory - Intact
- Speech - slurred
Cranial nerve examination
• 1 - olfactory sense - normal
• 2- visual acuity present,
• 3,4,6 - no ptosis Or nystagmus
• 5- corneal reflex present
• 7- no deviation of mouth, no loss of nasolabial folds, forehead wrinkling present
• 8- Normal hearing
• 9,10- position of uvula is central ,Gag reflex- present
• 11- sternocleidomastoid contraction present
• 12- no deviation of tongue
Motor system
Reflexes
Right Left
Biceps 3+ 3+
Triceps 3+ 3+
Knee. 3+. 3+
Ankle. 2+ 2+
Plantars- Extension Extension
Power. Lt. Rt
Upper limb -4/5. 4/5
Lower limb -4/5 4/5
TONE. Lt. Rt
Upper limbs N N
Lower limbs N N
No Involuntary movements
SENSORY SYSTEM
I – SPINOTHALAMIC R L
1. Crude touch N N
2. Pain. N. N
3. Temperature. N. N
II – POSTERIOR COLUMN
1. Fine touch. N. N
2. Vibration. N. N
3. Position sense. N. N
III – CORTICAL
1. Two point
discrimination. N. N
2. Tactile localisation. N. N
CEREBELLAR Tests
Finger Nose test - normal
Heel Knee test - normal
CVS; S1S2 +,No murmurs
RS :Bilateral air entry present
Normal vesicular breath sounds heard
Provisional diagnosis
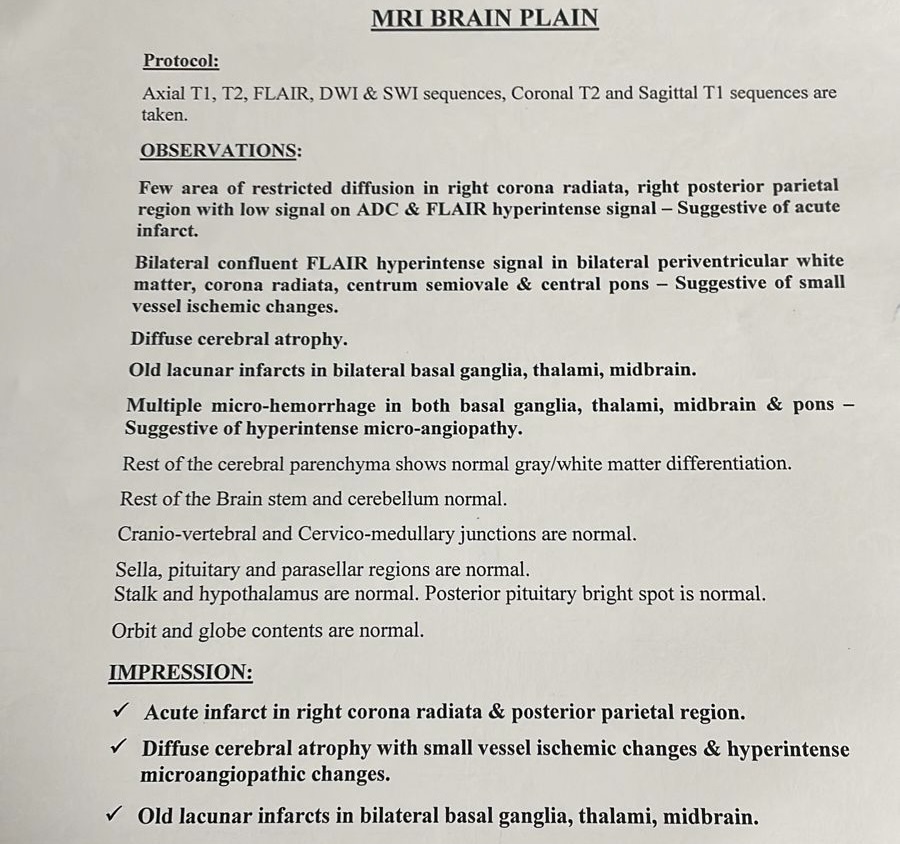
ACUTE CVA (ACUTE INFARCT IN RIGHT PARIETAL REGION) WITH SEIZURES (GENERALIZED TONIC SEIZURES)
Investigations







final diagnosis
ACUTE ISCHEMIC INFARCT VASCULAR DEMNTIA
ACUTE CVA ACUTE INFARCT IN RIGHT PARIETAL REGION WITH SEIZURES (GENERALIZED TONIC SEIZURES) 20 DAYS AGO
WITH IRON DEFICIENCY ANEMIA
treatment.
1) INJ . LEVIPIL 500 mgIV/BD
3) Tab. ECOSPRIN 75 mg
4) Tab. ATORVAS 40mg
5) TAB. OROFER- XT
6) INJ . PANTOP 40 MG



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}